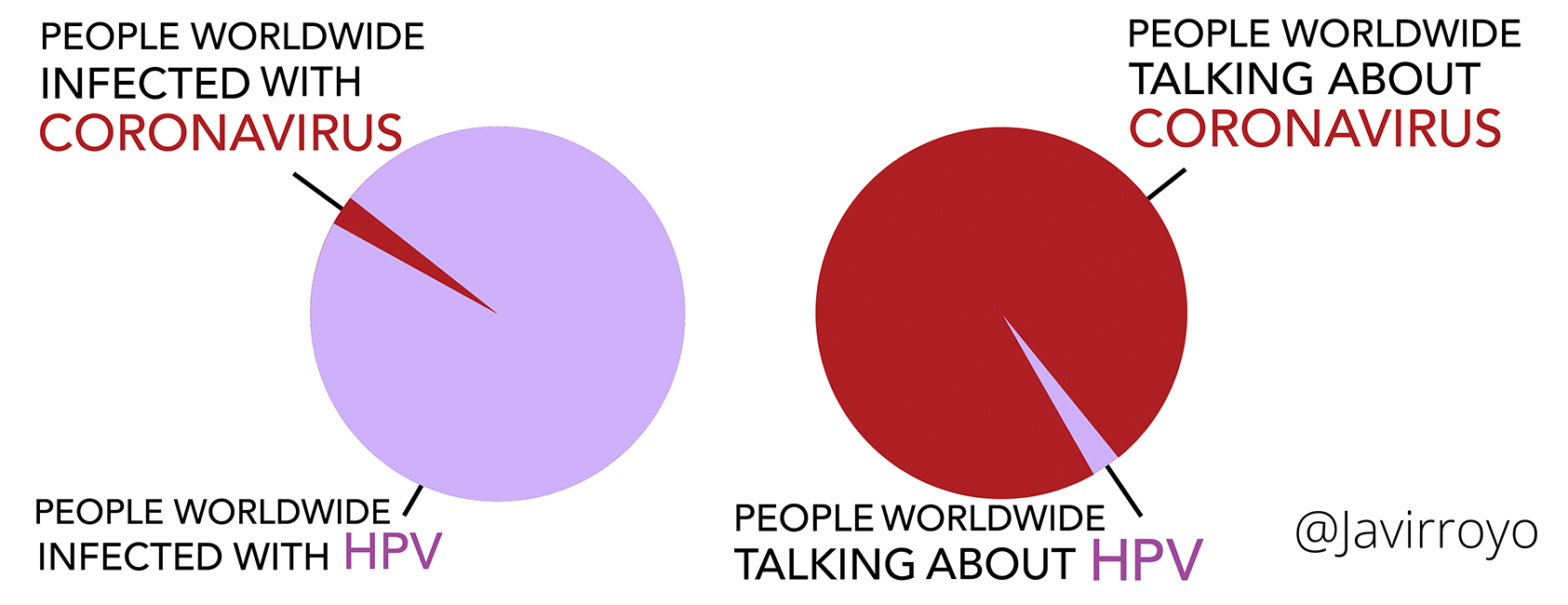
The image above perfectly illustrates what happens to other health issues during a pandemic. COVID-19 has inflicted grave injuries on our health care system, including a long list of essential services that fall under the umbrella of sexual health care.
Prevention services, such as school-based HPV vaccination programs, cervical and breast cancer screening, STI testing and screening, colposcopy, and numerous other sexual health services have been blindly sidelined since the start of the pandemic. This development is particularly troubling because these public health services reach at-risk and underserved groups, many of which already bear the brunt of this pandemic and represent a large proportion of cervical cancer cases in Canada.
We are starting to see the damage done to our communities and health care workforce from the effects of loss, trauma, precarious employment, and other stressors. Lessons must be learned and assimilated now to ensure that, in the future, sexual health and other essential services are insulated from the distorting effects of a similar systemic health crisis.
Health care systems have made unprecedented steps towards convenient, patient-centred, at-home cancer care during the pandemic. Additionally, faced with a concrete global need, telehealth has proven itself to be an effective means of care delivery in many situations. With respect to HPV, COVID chatbots have recently demonstrated potential to address patient information needs and frequently asked questions, which offloads and reduces clinician burden. These innovative and long overdue programs need to remain after the pandemic is over.
Online tools will need to evolve in terms of bandwidth, security, and delivery, which are still lacking in many sectors. Our vulnerable populations will require special accommodation since not all have access to cellphones or computers or have the literacy skills needed to access these tools. These emerging challenges should be addressed with great alacrity to prepare for other (un)foreseeable health, economic, and environmental crises that may be on the horizon. Investing time into these innovative technologies and targeted community-based solutions now will ensure that the needs of our communities will be met in an expected second wave and in new ‘global health crisis.’
There is a need for clinical guidance and resources for STI prevention programs that outline how to provide effective care when facility-based services and in-person, patient–clinician contact is limited. The accuracy of triage algorithms is constantly being improved thanks to deep learning and artificial intelligence so that patients can be directed to the appropriate resources and level of care. In preparation for any forthcoming surge or crisis, clinical guidance should cover patient prioritization, phone- or telemedicine-based triage, and leveraging other clinics and/or pharmacies to ensure patients continue to receive needed vaccinations, prescriptions, and treatment.
It’s vital we start treating health equity as an emergency rather than a statistic. The time is now to explore innovative data sources that do not allow technological advancements to leave our underserved communities behind. We need to better understand the sexual health burdens and implications of the COVID-19 pandemic to gain insight into the public’s health concerns and discussions regarding new technologies, partnering patterns, and questions about sexual health.
The current strategy of top-down decision-making is neither productive nor effective. Health care transformation that reflects the following principles will ensure sustainability and resiliency of HPV-related programs and services moving forward.
Firstly, we must explore new ways of working. Task shifting, as described by the World Health Organization (WHO), ensures a more efficient use of human resources when they are in short supply, which is a predominant issue in an epidemic.
Secondly, we must enable the front line because we know it is possible to improve health care communication in communities. For example, specific HPV prevention tasks, such as recruitment, enrolment in self-sampling or home testing, and vaccine education can be delegated to less specialized health care workers by implementing true partnerships with community health leaders/workers, especially during a time of crisis. They are best positioned to provide viable community-based solutions that address social risk factors and that begin to break down barriers to trust that are so embedded in socially disadvantaged communities dealing with COVID-19.
Finally, and most importantly, we must ensure that financial, human, and material resources are more equitably distributed in order to ensure that the strategic planning around COVID-19 does not obliterate other health care priorities like the WHO’s goal to set countries on the path to cervical cancer elimination. The Black Lives Matter protests have shown us that serious societal problems don’t just go away in the midst of a pandemic. The same principle applies to HPV.
We have safe and effective HPV vaccines, as well as innovative HPV testing and screening procedures to help us meet our important and attainable goals for the prevention of HPV and its related cancers. It’s time to seize the opportunity to meet our obligations nationally and internationally, to prioritize vulnerable populations, and think outside the box and reconsider the poorly executed health intervention strategies that are impeding clearly foreseeable successes. Creating a plan now, through online tools, task shifting, and wide access to resources, will help ensure that a second wave of COVID-19 or another future health crisis does not wreak havoc on other vulnerable sectors of the health care system, like cervical cancer screening, which we believe is too frequently trivialized.